doi: 10.58763/rc2025491
Review Article
Enhancing cognitive reserve: Evidence-based strategies for healthy aging
Fortalecer las reservas cognitivas: Estrategias basadas en evidencia para un envejecimiento con bienestar
Alicia Lianne García González1 ![]() *, Diego D. Díaz-Guerra2
*, Diego D. Díaz-Guerra2 ![]() *, Zoylen Fernández-Fleites3
*, Zoylen Fernández-Fleites3 ![]() *, Yunier Broche-Pérez4
*, Yunier Broche-Pérez4 ![]() *
*
ABSTRACT
Introduction: the concept of cognitive reserve (CR) emerges as a key explanatory framework by demonstrating that modifiable factors such as education, physical activity, and social participation can compensate for age-related cognitive decline. However, significant gaps persist in its practical implementation, especially in diverse community and political contexts.
Objective: this study aimed to analyze the most effective strategies to strengthen CR, integrating recent evidence and proposing a multilevel model that articulates individual, community, and structural interventions.
Methodology: a mixed-methods approach was adopted, combining systematic reviews with bibliometric analyses using VOSviewer, examining a total of 1060 studies organized into three axes: protective factors (693 studies), structured interventions (71 studies), and social determinants (296 studies).
Results: the results revealed that physical activity and education are the best-documented factors, showing robust associations with improved cognitive function. In contrast, bilingualism emerged as an under-researched area despite its neuroprotective potential.
Conclusions: the most effective interventions were multimodal approaches, such as the combination of cognitive training with physical exercise, while at the social level, community participation emerged as a key predictor of cognitive resilience, although marked disparities were observed between urban and rural areas.
Keywords: ageing, neuropsychology.
JEL Classification: I12, I30
RESUMEN
Introducción: el concepto de reserva cognitiva (RC) surge como un marco explicativo clave al demostrar que factores modificables como la educación, la actividad física y la participación social pueden compensar el deterioro cognitivo asociado a la edad. Sin embargo, persisten importantes brechas en su implementación práctica, especialmente en contextos comunitarios y políticos diversos.
Objetivo: analizar las estrategias más efectivas para fortalecer la RC, integrando evidencia reciente y proponiendo un modelo multinivel que articule intervenciones individuales, comunitarias y estructurales.
Metodología: se adoptó una metodología mixta que combinó revisiones sistemáticas con análisis bibliométricos mediante VOSviewer, examinando un total de 1060 estudios organizados en tres ejes: factores protectores (693 estudios), intervenciones estructuradas (71 estudios) y determinantes sociales (296 estudios).
Resultados: los resultados revelaron que la actividad física y la educación son los factores mejor documentados, mostrando asociaciones robustas con la mejora de la función cognitiva. En contraste, el bilingüismo apareció como un área subestudiada pese a su potencial neuroprotector.
Conclusiones: las intervenciones más eficaces fueron las multimodalidades, como la combinación de entrenamiento cognitivo con ejercicio físico, mientras que, a nivel social, la participación comunitaria emergió como un predictor clave de resiliencia cognitiva, aunque con marcadas disparidades entre zonas urbanas y rurales.
Palabras clave: envejecimiento, neuropsicología.
Clasificación JEL: I12, I30
Received: 07-02-2025 Revised: 15-05-2025 Accepted: 16-06-2025 Published: 31-07-2025
Editor: Alfredo
Javier Pérez Gamboa ![]()
1Universidad de Camagüey Ignacio Agramonte Loynaz. Camagüey, Cuba.
2Universidad Central Marta Abreu de Las Villas. Villa Clara, Cuba.
3Iniciativa Cubana en Salud Cognitiva. Villa Clara, Cuba.
4Prisma Behavioral Center. Florida, Estados Unidos de America.
Cite as: García González, A. L., Díaz-Guerra, D. D., Fernández-Fleites, Z. y Broche-Pérez, Y. (2025). Fortalecer las reservas cognitivas: Estrategias basadas en evidencia para un envejecimiento con bienestar. Región Científica, 4(2), 2025491. https://doi.org/10.58763/rc2025491
INTRODUCTION
Population aging poses urgent challenges for healthcare systems, especially in the area of cognitive decline and neurodegenerative diseases, according to Garbarino et al. (2022) and Boyle et al. (2021). Among these, Selkoe (2024) points out that Alzheimer's disease and other forms of dementia represent a growing burden for both individuals and societies.
Against this backdrop, the concept of cognitive reserve (CR) has gained relevance as an explanatory framework for the differences in how people cope with age-related brain changes (Grady et al., 2019; Soldan & Pettigrew, 2019). According to Radanovic (2020), this construct refers to the brain's adaptive capacity to compensate for damage through alternative neural networks or more efficient cognitive processes.
Crucially, according to Miraglia et al. (2024) and Zorec & Verkhratsky (2024), this reserve is not fixed but dynamic. This means that it is malleable through factors such as education, environment, and lifestyle habits.
Current research supports the idea that CR is nurtured by intellectually stimulating experiences throughout life (Ghamsari et al., 2024). Formal education, lifelong learning, and participation in complex social activities act as pillars in its construction (Ponniah & Savarimuthu, 2024; Stern, 2021).
However, cognitive enrichment is not limited to the intellectual. Bialystok (2021) and Bennet et al. (2019) reveal that bilingualism, regular physical exercise, and dietary patterns such as the Mediterranean diet also strengthen brain resilience. These findings point to a fundamental principle according to Nishimune & Inoue (2023), who state that neuronal plasticity persists into old age, allowing the brain to reorganize itself in response to new stimuli.
However, a challenge remains. Despite the consensus on the factors that promote CR, there is still a lack of clarity on how to implement this knowledge in public policies or community interventions (Morone et al., 2020). However, a growing group of authors emphasizes the need to create environments that facilitate active aging at the population level (Daw et al., 2022).
Given the global increase in cognitive disorders and the socioeconomic costs they entail, developing evidence-based strategies to enhance CR is not only desirable but urgent (Dunstan et al., 2021; Lee et al., 2023). This article arises from the need to integrate disparate findings and critically evaluate which interventions can be transferred to real-life contexts with sociocultural diversity. Its objective is to analyze the most effective strategies supported by recent literature. Furthermore, it proposes the conceptualization of an integrative model that combines cognitive stimulation, healthy habits, and social participation.
METHODOLOGY
This research adopted a mixed methodological approach that combined documentary reviews with bibliometric analysis (Sánchez Castillo et al., 2024). This design allowed for the identification of trends in the scientific literature, the evaluation of the robustness of existing interventions, and the synthesis of key findings for the construction of the proposed model.
Search strategy, analysis and conceptual mapping
A comprehensive search was conducted in multidisciplinary databases (PubMed, Scopus, Web of Science, and PsycINFO) to retrieve studies published between 2019 and 2024. Using VOSviewer software (Mojica et al., 2021), a term co-occurrence analysis was performed to identify dominant thematic clusters in the literature. This analysis was performed based on three filters, which, in turn, constituted the main research axes:
· Protective factors (education, bilingualism, physical activity). 693 studies were identified using the formula: ("cognitive reserve" OR "brain resilience" OR "neuroprotection”) AND ("protective factors" OR "protective mechanisms" OR "modifiable factors”) AND ("education" OR "educational attainment" OR "lifelong learning" OR "bilingualism" OR "multilingualism" OR "physical activity" OR "exercise" OR "aerobic training" OR "motor activity”) AND ("aging" OR "older adults" OR "elderly" OR "cognitive aging").
· Structured interventions (computerized cognitive training, multidomain therapies). 71 studies were identified using the formula: ("cognitive reserve" OR "cognitive resilience" OR "brain plasticity”) AND ("structured interventions" OR "cognitive training" OR "computerized training" OR "cognitive rehabilitation" OR "multidomain interventions" OR "combined therapies”) AND ("working memory training" OR "processing speed training" OR "dual-task training" OR "exergaming" OR "cognitive stimulation therapy”) AND ("clinical trial" OR "randomized controlled trial" OR "longitudinal study").
· Social determinants (support networks, public policies). 296 studies were identified using the formula: ("cognitive reserve" OR "cognitive aging" OR "successful aging”) AND ("social determinants" OR "social support" OR "community engagement" OR "social networks" OR "public policies" OR "health policies" OR "aging-friendly environments”) AND ("social participation" OR "volunteering" OR "intergenerational programs" OR "urban design" OR "age-friendly cities”) AND ("gerontology" OR "social epidemiology" OR "public health").
Discussion of findings and development of the model
To discuss the findings from the literature reviewed, an interpretive approach was adopted that prioritized three key dimensions: consistency of results, practical applicability, and theoretical soundness of the identified interventions. Based on this discussion of results, a conceptual framework was constructed that organizes the strategies into three levels of action:
· Micro (individual habits such as lifelong learning and physical exercise).
· Meso (intergenerational community programs and support networks).
· Macro (urban design and public policies that facilitate active aging).
RESULTS AND DISCUSSION
Conceptual mapping
Protective factors
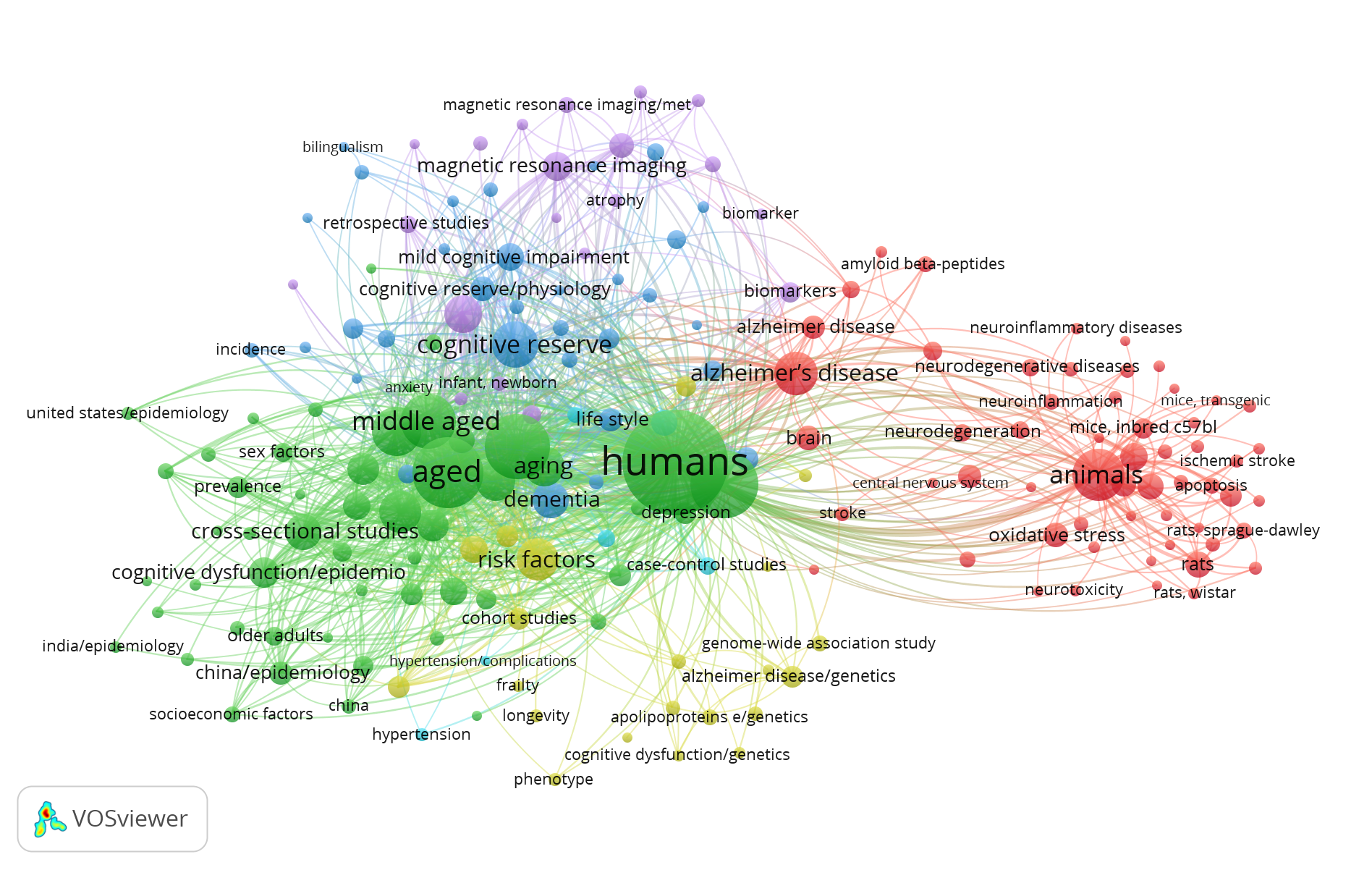
The results of the keyword co-occurrence analysis (figure 1) show that the term "cognitive reserve" appears with a frequency of 82 occurrences and a total link strength of 642, positioning it as a central concept in this area of research. This construct shows strong associations with "cognition" (95 occurrences, 767 link strength) and "cognitive dysfunction" (28 occurrences, 249 link strength), highlighting its fundamental role in studies on healthy brain aging.
Among the most researched protective factors, three main categories clearly stand out. First, physical activity, represented by terms such as "exercise" (22 occurrences, 189 link strength) and "physical activity" (9 occurrences, 89 link strength), which show particularly robust links with "cognitive aging" (18 occurrences, 152 link strength).
Second, educational aspects appear as another important pillar, with "educational status" (27 occurrences, 257 link strength) and "education" (15 occurrences, 145 link strength) significantly correlated with "cognitive reserve/physiology" (24 occurrences, 256 link strength). Finally, although less represented, factors such as bilingualism and multilingualism emerge ("bilingualism" with 5 occurrences and 44 link strength; "multilingualism" with 8 occurrences and 75 link strength), which appear associated with specific cognitive functions such as "executive function" (13 occurrences, 92 link strength).
|
Figure 1. Keyword co-occurrence network on cognitive reserve and protective factors |
|
|
Source: own elaboration based on VOSviewer
Research in this period shows a clear focus on older populations, as evidenced by the high frequencies of terms such as "aged" (196 occurrences, 1823 link strengths) and "older adults" (15 occurrences, 112 link strengths). Particularly relevant is the strong association with conditions such as "mild cognitive impairment" (29 occurrences, 259 link strengths) and "Alzheimer's disease" (74 occurrences, 553 link strengths), reflecting the interest in understanding protective factors in contexts of cognitive decline.
At the level of biological mechanisms, terms such as "neuroprotection" (24 occurrences, 143 link strengths) and "oxidative stress" (25 occurrences, 115 link strengths) frequently appear alongside "lifestyle" (6 occurrences, 64 link strengths), highlighting the interactions between modifiable habits and biomolecular processes.
The analysis also reveals important gaps in the literature. Bilingualism, despite its potential as a protective factor, has a significantly lower density of studies compared to other factors. Furthermore, the low co-occurrence between "social class" (7 occurrences, 69 link strengths) and protective factors indicates an important area of opportunity for investigating how social inequalities can affect access to interventions that promote cognitive reserve. The methodological data show a predominance of cross-sectional studies (50 occurrences, 488 link strengths) over longitudinal studies (40 occurrences, 378 link strengths), suggesting the need for further research to establish causal relationships.
These findings have important implications for future research. The clear consensus on physical activity and education as fundamental pillars of cognitive reserve contrasts with the need to delve deeper into other potential protective factors. Integrating protective factors (17 occurrences, 158 link strengths) into more comprehensive multifactorial models could help bridge the gap between basic research and practical applications.
Structured interventions
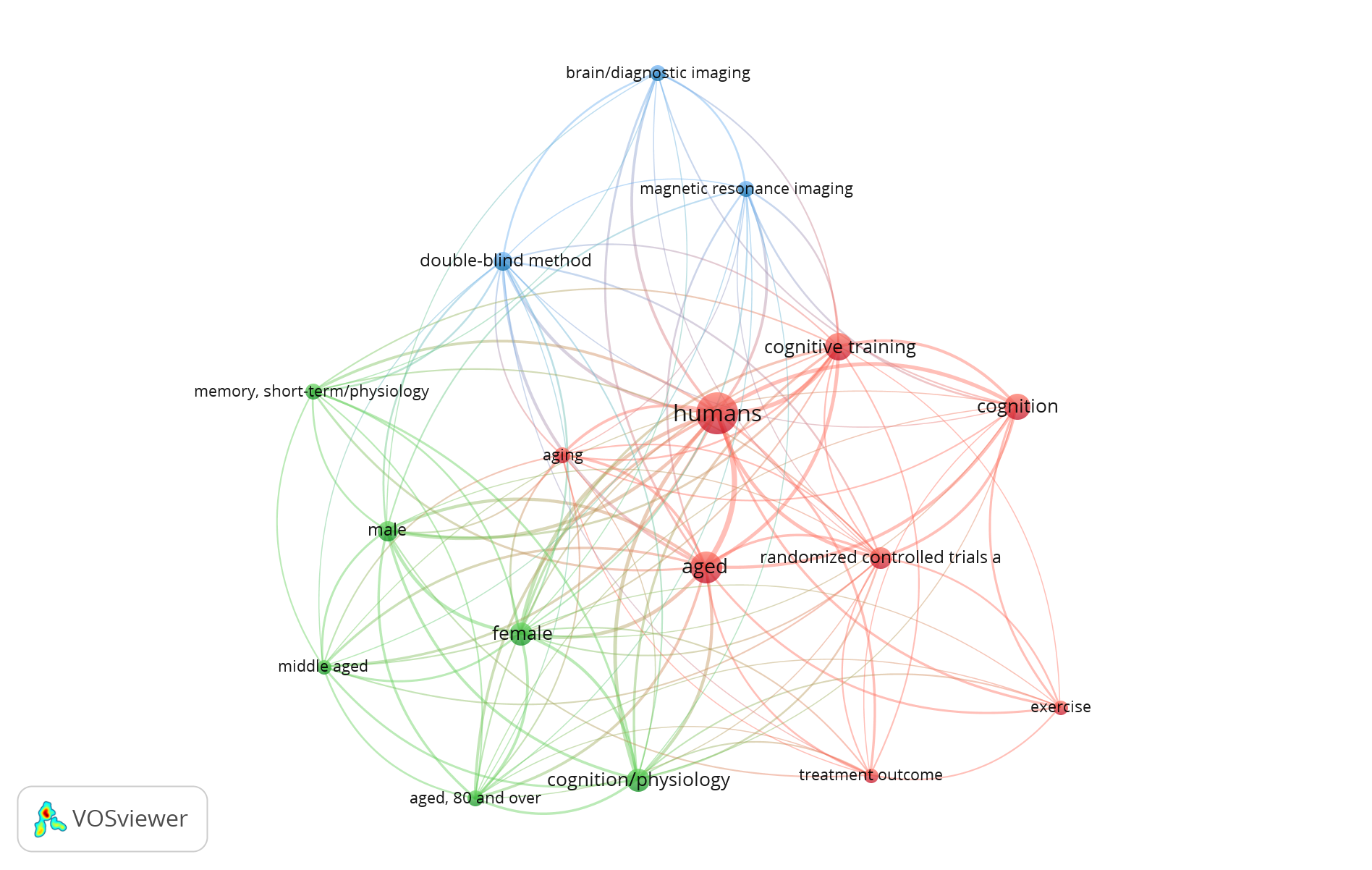
The data from the keyword co-occurrence analysis (figure 2) show that cognitive training emerges as the most studied intervention, with 17 occurrences and a total link strength of 67. This technique is frequently associated with improvements in basic cognitive processes, particularly in "memory, short-term/physiology" (6.32) and "cognition/physiology" (11.62).
The primary target populations are older adults, as evidenced by the high frequencies of "aged" (22.113) and "aged, 80 and over" (6.43), with a particular interest in evaluating the effects of training on general cognition ("cognition" = 14.50). The predominant methodological designs include randomized controlled trials, as evidenced by the presence of randomized controlled trials (10.46) and double-blind methods (8.41), reflecting the scientific rigor applied in this area of research.
The results show that structured interventions are frequently complemented with neuroimaging assessments, where brain/diagnostic imaging (6.24) and magnetic resonance imaging (6.28) appear as key tools for measuring neurobiological changes. Although less represented, physical activity ("exercise" = 5.23) emerges as a supporting component in some intervention protocols.
|
Figure 2. Keyword co-occurrence network on cognitive reserve and structured interventions |
|
|
Source: own elaboration based on VOSviewer
The gender distribution in the studies shows a slight predominance of female samples ("female" = 11.70) over male samples ("male" = 9.59). The term "treatment outcome" (5.24) appears with moderate frequency, suggesting a growing interest in standardizing the effectiveness measures of these interventions.
This analysis reveals two areas that require greater attention in future research: first, the need to include more diverse populations in terms of age, particularly middle-aged groups (5.36), for early preventive strategies. Second, the opportunity to integrate more multimodal components into intervention protocols, combining cognitive training with other proven effective strategies. The data support the validity of structured cognitive training as a tool to strengthen cognitive reserve, although they point out the importance of tailoring interventions according to individual characteristics and the specific cognitive domains to be improved.
Social determinants
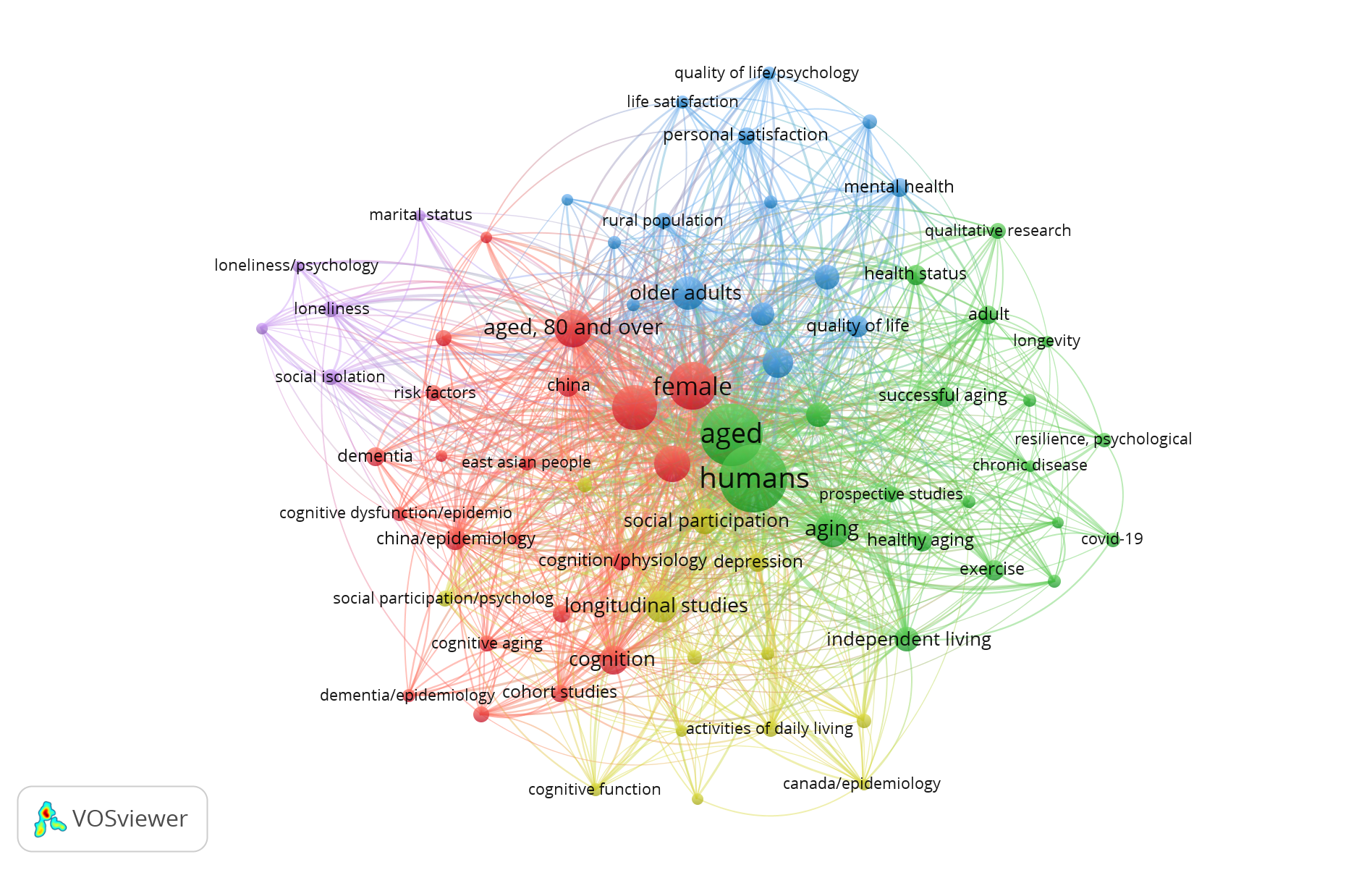
The results of the keyword co-occurrence analysis for this search formula are presented in figure 3. The term "cognitive reserve" appears with 10 occurrences and a link strength of 60, demonstrating its fundamental association with psychosocial factors such as "social participation" (22.183) and "social support" (17.154). These findings underscore the crucial role that social connections play in maintaining cognitive health during aging.
The results show a marked positive correlation between active social participation and indicators of cognitive well-being. Particularly relevant is the association of "social participation/psychology" (9.104) with "quality of life" (16.126) and "healthy aging" (13.105), suggesting that social engagement protects cognitive function and also contributes to healthier aging. In contrast, social isolation emerges as a significant risk factor, with "social isolation" (9.76) and "loneliness" (9.70) showing negative correlations with markers of cognitive reserve.
Although less studied in comparison, socioeconomic factors reveal their importance through terms such as "socioeconomic factors" (5.49) and "social class" (5.39), which appear to be linked to higher risks of cognitive impairment (9.87). These associations point to potential disparities in access to resources that support brain health, highlighting the need to address social inequalities as an integral part of prevention strategies.
|
Figure 3. Keyword co-occurrence network on cognitive reserve and social determinants |
|
|
Source: own elaboration based on VOSviewer
Geographic and cultural differences emerge as another relevant focus of research. Studies in East Asia, represented by "East Asian people" (7.80) and "China/epidemiology" (15.154), contrast with findings in North American contexts ("Canada/epidemiology" = 5.40), which could reflect variations in cultural models of aging and social support systems. This diversity emphasizes the importance of developing contextualized approaches to strengthening cognitive reserve.
From a methodological perspective, longitudinal studies ("longitudinal studies" = 34.321) predominate over cross-sectional designs ("cross-sectional studies" = 29.236), indicating a growing interest in understanding the long-term trajectories of cognitive decline in relation to social determinants. In addition, qualitative approaches ("qualitative research" = 9.60) provide valuable insights into subjective dimensions such as "social networks" (5.38) and "psychological resilience" (7.49), enriching the understanding of the psychosocial mechanisms involved.
The most studied populations include older adults ("aged" = 124.981; "older adults" = 35 256), people in the transition to retirement ("retirement" = 7.51), and rural residents ("rural population" = 9.87). These research focuses reflect current priorities in social gerontology, although they also highlight important gaps, particularly with regard to disadvantaged socioeconomic groups and multicultural populations.
The COVID-19 pandemic ("covid-19" = 7.40) is emerging as a disruptive factor that has reshaped social dynamics and its impact on cognitive health, although its study in this specific context remains incipient. This situation underscores the need for research exploring the long-term effects of enforced social distancing on cognitive reserve in vulnerable populations.
Proposed conceptual model
Micro Level: Individual factors in the construction of cognitive reserve
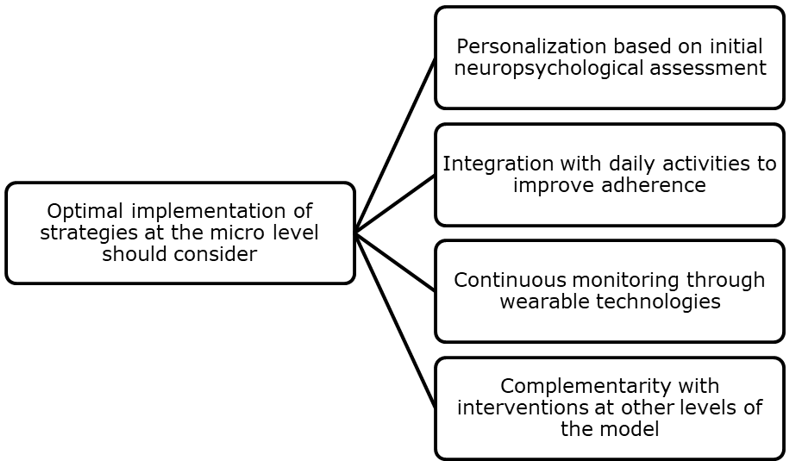
The micro level of the proposed model focuses on modifiable factors at the individual level that contribute to strengthening cognitive reserve, supported by the converging findings of the three bibliometric searches conducted (figure 4). The data reveal that the individual strategies with the greatest evidence cluster into three interconnected domains: physical activity, cognitive stimulation, and healthy habits, which show synergistic effects when implemented consistently.
Physical activity emerges as the best-documented individual factor (Arida & Teixeira-Machado, 2021; González-García et al., 2023). Aerobic exercise, in particular ("exercise" = 22 occurrences in search 2, link strength = 189), appears consistently associated with improvements in "cognitive function" (6.57) and "cognitive reserve/physiology" (24.256) according to Gelfo et al. (2022).
The underlying neurobiological mechanisms include increased cerebral blood flow and hippocampal neurogenesis, which are particularly relevant for counteracting cognitive aging (18.152) (Webb et al., 2021). However, the analysis shows that optimal benefits require moderate-to-high intensity and a minimum frequency of 150 minutes per week, according to the reviewed longitudinal results ("longitudinal studies" = 40, 378) (Huang et al., 2024; Yu et al., 2022).
In the area of cognitive stimulation, structured training ("cognitive training" = 17.67) demonstrates efficacy, especially for executive functions ("executive function" = 13.92) and working memory ("memory, short-term/physiology" = 6.32) (Andrews et al., 2019). However, the results highlight that its effectiveness increases significantly when combined with physical activity (co-occurrence "exercise+cognitive training" = 9.78), supporting the multimodal approach (Held et al., 2022). Bilingualism ("bilingualism" = 5.44) and continuous learning ("education" = 15.145) appear as complementary strategies that promote greater cognitive flexibility, as pointed out by Bialystok (2021) and Bennet et al. (2019), although with less representation in recent literature.
|
Figure 4. Implications for micro-level implementation |
|
|
Source: own elaboration
Healthy lifestyle habits complete the triangle of micro-level interventions. The Mediterranean diet, according to Berendsen et al. (2019) and Tan et al. (2022), shows consistent associations with a lower risk of cognitive dysfunction (28.249). Furthermore, adequate sleep patterns emerge as an underestimated protective factor (Deary et al., 2019; Dupre, 2022).
Current evidence indicates that long-term adherence constitutes the main challenge for interventions at this level. Health behavior data (5.46) obtained by Luque-Casado et al. (2021) indicate that adherence to physical exercise in older adults is affected by several variables, including exercise program characteristics, professional involvement, supervision, technology, and participant education.
Meso-Level: Community networks and environments that facilitate healthy cognitive aging
The meso-level of the integrative model addresses the community and social factors that act as catalysts for cognitive reserve. The results of the three bibliometric searches reveal that this level is particularly relevant for sustaining the benefits of long-term interventions, with a demonstrated impact on reducing the risk of cognitive decline (figure 5).
In this sense, the data show that active social participation ("social participation" = 22 occurrences, link strength = 183) emerges as one of the most consistent predictors of cognitive reserve in older adults, according to Bäckman et al. (2022) and Jaeggi & Waever (2021). Furthermore, Spalding et al. (2021) point out that intergenerational programs have been shown to improve executive function ("executive function" = 13.92) (Zhong et al., 2020) and emotional well-being ("life satisfaction" = 6.53) (Pérez Valdivia et al., 2024).
These findings are reinforced by the strong association between "social support" (17.154) and a lower prevalence of dementia ("dementia" = 11.66) (Power et al., 2021). In this regard, Larson et al. (2023) corroborate that greater social participation in middle and old age is associated with a 30-50% lower risk of dementia, possibly due to increased cognitive reserve and brain maintenance through stress reduction and improved cerebrovascular health.
|
Figure 5. Implications for the implementation of the meso level |
|
|
Source: own elaboration
Bibliometric analysis identifies that physical and social environments play a determining role. Communities with greater opportunities for social engagement, such as accessible cultural centers, structured volunteer programs, and safe public spaces, have lower rates of social isolation ("social isolation" = 9.76) (Fujiwara et al., 2019). It is noteworthy that Holmes et al. (2019) argue that in rural contexts ("rural population" = 9.87), where access to specialized services is limited, informal support networks ("social networks" = 5.38) partially compensate for this deficiency. However, significant disparities persist compared to urban areas.
Macro Level: public policies and structural determinants of cognitive reserve
The macro level of the integrative model examines how political, economic, and social systems influence cognitive reserve at the population level (figure 6). Bibliometric analyses reveal that this level takes on particular relevance in the post-pandemic context, where inequalities in healthy cognitive aging have widened.
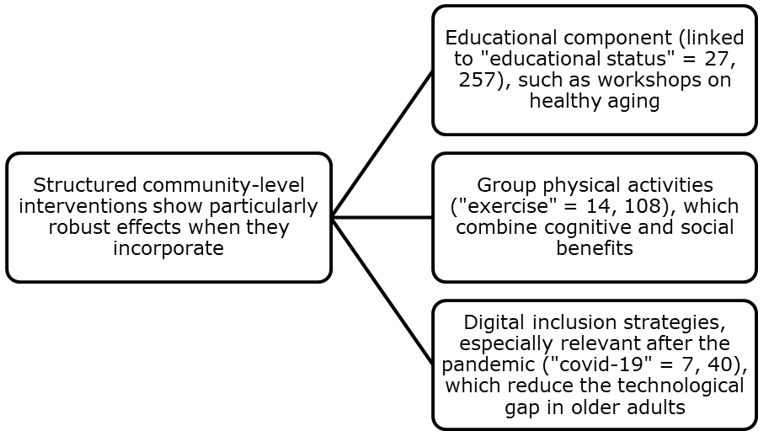
Data show that nations with integrated active aging policies ("successful aging" = 14.108) perform better on key brain health indicators (Lucantoni et al., 2023). This highlights the fundamental role of policy decisions in promoting cognitive well-being (González Argote et al., 2024).
Furthermore, research shows that the most effective policies combine targeted interventions with structural changes. National cognitive stimulation programs ("cognitive training" = 17.67), when implemented alongside improvements in urban infrastructure ("residence characteristics" = 5.42) and social protection systems ("retirement" = 7.51), significantly reduce the incidence of cognitive decline, as was the case with Kua et al. (2022) in Singapore.
However, the analysis reveals worrying disparities between regions and socioeconomic groups. Populations with lower educational levels ("educational status" = 27.257) and greater material deprivation ("socioeconomic factors" = 5.49) show a significantly higher prevalence of early cognitive problems (Chauvel et al., 2021; Tan & Tan, 2023). These findings underscore the need to address structural inequalities as an essential part of any strategy to strengthen cognitive reserve at the population level.
Urban design emerges as a determining factor at this macro level. In this regard, the studies by Assem et al. (2023) and Abbas et al. (2024) stand out, highlighting that cities that incorporate principles of neuroarchitecture and universal accessibility demonstrate measurable improvements in cognitive health indicators.
According to Dong et al. (2024), green spaces, accessible transportation, and environments that encourage social interaction appear consistently associated with greater physical activity ("physical activity" = 6.57), less social isolation ("social isolation" = 9.76), and better cognitive performance ("cognitive function" = 6.57) in older adults. These findings support the importance of considering the cognitive dimension in urban planning and territorial development policies (Veeroja et al., 2022).
|
Figure 6. Implications for macro-level implementation |
|
|
Source: own elaboration
Within the health systems framework, integrating routine cognitive assessments into primary care has proven to be a cost-effective strategy (Thompson, 2024). When these assessments are combined with educational campaigns ("health behavior" = 5.46) and universal access to preventive interventions ("prevention" = 11.86), significant improvements are observed in the early detection and management of cognitive decline (Pugh et al., 2024).
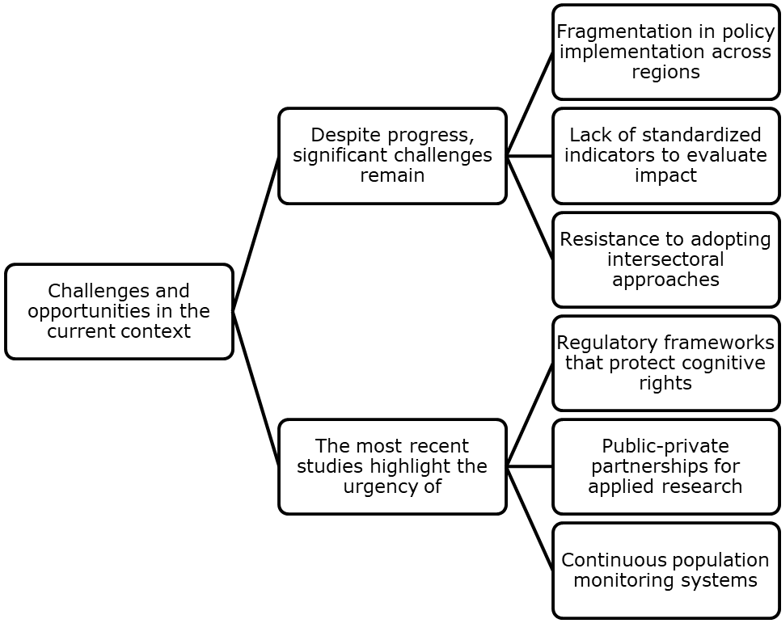
On the other hand, Awata (2024) highlights the urgency of developing regulatory frameworks that specifically protect the cognitive rights of older adults ("healthy aging" = 13.105). This includes policies that guarantee access to evidence-based interventions, protect against age discrimination in the workplace, and promote continued social inclusion (Warhurst & Black, 2024).
This macro-level completes the integrative model by providing the structural framework necessary for individual and community interventions to reach their full potential. The challenge for the coming years is to translate these findings into concrete policies that can be adapted to diverse cultural and socioeconomic contexts. This will ensure that the benefits of healthy cognitive aging are accessible to the entire population.
CONCLUSIONS
The evidence analyzed confirms that cognitive reserve is a dynamic and multifactorial construct influenced by elements operating at different levels. At the individual level, regular physical activity, continuous cognitive stimulation, and healthy habits constitute the foundation for building brain resilience, although their effectiveness largely depends on long-term adherence and the personalization of interventions. However, these individual efforts are insufficient without a community environment to support them, as demonstrated by the positive impact of intergenerational programs and accessible social spaces in reducing isolation and cognitive decline.
At the macro level, public policies play a decisive role in creating structural conditions that favor active aging, from inclusive urban design to health systems that integrate routine cognitive assessments. Despite these advances, critical challenges persist, such as socioeconomic gaps that limit access to protective resources and the limited research on rural and multicultural populations. Future courses of action should prioritize equity, combining evidence-based interventions with technological innovations and regulatory frameworks that protect the cognitive rights of older adults. Ultimately, this comprehensive approach will not only enrich scientific research but also offer practical tools for building more inclusive and resilient societies in the face of population aging.
REFERENCES
Abbas, S., Khattar, Z., Sabatier, J., Okdeh, N., Kovacic, H., Fajloun, Z., & Roufayel, R. (2024). Neuroarchitecture: How the Perception of Our Surroundings Impacts the Brain. Biology, 13. https://doi.org/10.3390/biology13040220
Andrews, G., Murphy, K., & Nguyen, L. (2019). Immediate and long-term efficacy of executive functions cognitive training in older adults: A systematic review and meta-analysis. Psychological bulletin, 145 7, 698-733. https://doi.org/10.1037/bul0000196
Arida, R., & Teixeira-Machado, L. (2021). The Contribution of Physical Exercise to Brain Resilience. Frontiers in Behavioral Neuroscience, 14. https://doi.org/10.3389/fnbeh.2020.626769
Assem, H., Fathy, F., & Khodeir, L. (2023). Designing for human wellbeing: The integration of neuroarchitecture in design – A systematic review. Ain Shams Engineering Journal. https://doi.org/10.1016/j.asej.2022.102102
Awata, S. (2024). Living alone with dementia in Japan: challenges and policies. Alzheimer's & Dementia, 20. https://doi.org/10.1002/alz.087607
Bäckman, L., Patalay, P., Marseglia, A., Wang, H., Westman, E., Dekhtyar, S., Kalpouzos, G., Laukka, E., Maddock, J., & Welmer, A. (2022). Social Health and Cognitive Change in Old Age: Role of Brain Reserve. Annals of Neurology, 93. https://doi.org/10.1002/ana.26591
Bennett, D., Schneider, J., Boyle, P., Wilson, R., Lamar, M., & Yu, L. (2019). Education and cognitive reserve in old age. Neurology, 92, e1041 - e1050. https://doi.org/10.1212/WNL.0000000000007036
Berendsen, A., van den Brink, A., van de Rest, O., & Brouwer-Brolsma, E. (2019). The Mediterranean, Dietary Approaches to Stop Hypertension (DASH), and Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) Diets Are Associated with Less Cognitive Decline and a Lower Risk of Alzheimer's Disease—A Review. Advances in Nutrition, 10, 1040 - 1065. https://doi.org/10.1093/advances/nmz054
Bialystok, E. (2021). Bilingualism: Pathway to Cognitive Reserve. Trends in Cognitive Sciences, 25, 355-364. https://doi.org/10.1016/j.tics.2021.02.003
Boyle, P., Wilson, R., Yu, L., Arfanakis, K., Schneider, J., Bennett, D., Dawe, R., & Wang, T. (2021). To what degree is late life cognitive decline driven by age-related neuropathologies? Brain: a journal of neurology. https://doi.org/10.1093/brain/awab092
Chauvel, L., Leist, A., & Bar-Haim, E. (2021). Inequality of educational opportunity at time of schooling predicts cognitive functioning in later adulthood. SSM - Population Health, 15. https://doi.org/10.1016/j.ssmph.2021.100837
Daw, P., Wood, G., King, A., Pykett, J., Stathi, A., Agyapong-Badu, S., & Banchoff, A. (2022). The Role of Urban Environments in Promoting Active and Healthy Aging: A Systematic Scoping Review of Citizen Science Approaches. Journal of Urban Health: Bulletin of the New York Academy of Medicine, 99, 427 - 456. https://doi.org/10.1007/s11524-022-00622-w
Deary, I., Radakovic, R., Cox, S., Harris, S., Allerhand, M., Starr, J., Davies, G., Ritchie, S., Riha, R., Breen, D., & Hagenaars, S. (2019). Sleep and cognitive aging in the eighth decade of life. Sleep, 42. https://doi.org/10.1093/sleep/zsz019
Dunstan, D., Stathi, A., Dogra, S., Owen, N., Sugiyama, T., & Gardiner, P. (2021). Active Aging and Public Health: Evidence, Implications, and Opportunities. Annual review of public health. https://doi.org/10.1146/annurev-publhealth-052620-091107
Dupre, M., Wang, N., & Li, M. (2022). Association Between the Self-Reported Duration and Quality of Sleep and Cognitive Function Among Middle-aged and Older Adults in China. Journal of affective disorders. https://doi.org/10.1016/j.jad.2022.02.039
Fisher, M. (2023). Multi-sectoral action to promote psychological wellbeing: Theorising the role of place-based policy. Health promotion journal of Australia: official journal of Australian Association of Health Promotion Professionals. https://doi.org/10.1002/hpja.754
Fujiwara, Y., Ejiri, M., Ihara, K., Kim, H., Obuchi, S., Hirano, H., Ishii, K., Watanabe, Y., Kawai, H., & Oka, K. (2019). Social participation reduces isolation among Japanese older people in urban area: A 3-year longitudinal study. PLoS ONE, 14. https://doi.org/10.1371/journal.pone.0222887
Garbarino, V., Pollet, E., Palavicini, J., Kellogg, D., Kraig, E., Orr, M., & Gonzales, M. (2022). Biological aging processes underlying cognitive decline and neurodegenerative disease. The Journal of Clinical Investigation, 132. https://doi.org/10.1172/JCI158453
Gelfo, F., Petrosini, L., Mandolesi, L., Caltagirone, C., Serra, L., Balsamo, F., Bozzali, M., & Bonarota, S. (2022). Walking, Running, Swimming: An Analysis of the Effects of Land and Water Aerobic Exercises on Cognitive Functions and Neural Substrates. International Journal of Environmental Research and Public Health, 19. https://doi.org/10.3390/ijerph192316310
Ghamsari, A., Rezapour, T., Kormi-Nouri, R., Karsazi, H., & Hatami, J. (2024). Which intellectual activities are related to cognitive reserve? Introduction and testing a three-dimensional model. Psychological research. https://doi.org/10.1007/s00426-024-01926-z
González Argote, J., López Sánchez, A. A., Pérez Gamboa, A. J. (2024). Principales tendencias sobre salud mental en el campo de la Psicología: una revisión mixta en Scopus. PsiqueMag, 13(2), 35-55. https://doi.org/10.18050/psiquemag.v13i2.3135
Grady, C., Raz, N., Stern, Y., Jones, R., & Barnes, C. (2019). Brain reserve, cognitive reserve, compensation, and maintenance: operationalization, validity, and mechanisms of cognitive resilience. Neurobiology of Aging, 83, 124-129. https://doi.org/10.1016/j.neurobiolaging.2019.03.022
Holmes, S., Fields, N., Gibson, A., & Richardson, V. (2019). Providing Care for Persons with Dementia in Rural Communities: Informal Caregivers’ Perceptions of Supports and Services. Journal of Gerontological Social Work, 62, 630 - 648. https://doi.org/10.1080/01634372.2019.1636332
Huang, N., Wu, Y., Teo, W., Siew-Pin, J., & Chen, W. (2024). Identifying exercise and cognitive intervention parameters to optimize executive function in older adults with mild cognitive impairment and dementia: a systematic review and meta-analyses of randomized controlled trials. European Review of Aging and Physical Activity, 21. https://doi.org/10.1186/s11556-024-00357-4
Jaeggi, S., & Weaver, A. (2021). Activity Engagement and Cognitive Performance Amongst Older Adults. Frontiers in Psychology, 12. https://doi.org/10.3389/fpsyg.2021.620867
Kua, E., Goh, L., Ng, T., Chua, R., Mahendran, R., & Feng, L. (2022). A 5‐year community program in Singapore to prevent cognitive decline. Asia‐Pacific Psychiatry, 14. https://doi.org/10.1111/appy.12518
Larson, E., Sommerlad, A., Livingston, G., Shirai, K., Röhr, S., Singh‐Manoux, A., & Kivimäki, M. (2023). Social participation and risk of developing dementia. Nature Aging, 3, 532 - 545. https://doi.org/10.1038/s43587-023-00387-0
Lee, C., Portegijs, E., & Zhu, X. (2023). Activity-friendly environments for active aging: The physical, social, and technology environments. Frontiers in Public Health, 10. https://doi.org/10.3389/fpubh.2022.1080148
Lucantoni, D., Lamura, G., Barbabella, F., Socci, M., & Principi, A. (2023). Active Aging Policies Targeting Health and Care During the of COVID-19 Pandemic: A Systematic Review and Thematic Analysis of Italian National and Regional Policies. Journal of Applied Gerontology. https://doi.org/10.1177/07334648231182243
Luque-Casado, A., Gasque, P., Collado-Mateo, D., Fernández-Del-Olmo, M., Peñacoba, C., Del Coso, J., Amado-Alonso, D., Lavín-Pérez, A., & Leyton-Román, M. (2021). Key Factors Associated with Adherence to Physical Exercise in Patients with Chronic Diseases and Older Adults: An Umbrella Review. International Journal of Environmental Research and Public Health, 18. https://doi.org/10.3390/ijerph18042023
Miraglia, F., Rossini, P., Pappalettera, C., Carrarini, C., & Vecchio, F. (2024). Cognitive resilience/reserve: Myth or reality? A review of definitions and measurement methods. Alzheimer's & Dementia, 20, 3567 - 3586. https://doi.org/10.1002/alz.13744
Mojica, Z., Lennertz, L., & McAllister, J. (2021). Mapping A Discipline: A Guide to Using VOSviewer for Bibliometric and Visual Analysis. Science & Technology Libraries, 41, 319 - 348. https://doi.org/10.1080/0194262X.2021.1991547
Morone, P., Lopolito, A., Falcone, P., & Sica, E. (2020). A Combined method to model policy interventions for local communities based on people knowledge. MethodsX, 7. https://doi.org/10.1016/j.mex.2020.100877
Nishimune, H., & Inoue, R. (2023). Neuronal Plasticity and Age-Related Functional Decline in the Motor Cortex. Cells, 12. https://doi.org/10.3390/cells12172142
Pérez Valdivia, Y., Rojas Sánchez, G., Sánchez Castillo, V., & Pérez Gamboa, A. (2024). La categoría bienestar psicológico y su importancia en la práctica asistencial: una revisión semisistemática. Revista Información Científica, 103, e4478. https://doi.org/10.5281/zenodo.10615337
Ponniah, R., & Savarimuthu, A. (2024). Cognition and Cognitive Reserve. Integrative psychological & behavioral science. https://doi.org/10.1007/s12124-024-09821-3
Power, J., Shah, R., Joyce, J., Britt, C., Owen, A., Storey, E., Freak-Poli, R., Ryan, J., Hu, J., & Woods, R. (2021). Social isolation, social support, and loneliness and their relationship with cognitive health and dementia. International Journal of Geriatric Psychiatry, 37, 1 - 12. https://doi.org/10.1002/gps.5644
Pugh, M., Drahota, A., Udell, J., & Mackenzie, H. (2024). Psychological and educational interventions for preventing falls in older people living in the community. The Cochrane database of systematic reviews, 10, CD013480. https://doi.org/10.1002/14651858.CD013480.pub2
Radanovic, M. (2020). Cognitive reserve: an evolving concept. International Psychogeriatrics, 32, 7 - 9. https://doi.org/10.1017/S1041610219001947
Sánchez Castillo, V., Pérez Gamboa, A. J., & Gómez Cano, C. A. (2024). Trends and evolution of Scientometric and Bibliometric research in the SCOPUS database. Bibliotecas. Anales de investigación, 20(1). http://revistas.bnjm.sld.cu/index.php/BAI/article/view/834
Selkoe, D. (2024). The advent of Alzheimer treatments will change the trajectory of human aging. Nature aging, 4 4, 453-463. https://doi.org/10.1038/s43587-024-00611-5
Soldan, A., & Pettigrew, C. (2019). Defining Cognitive Reserve and Implications for Cognitive Aging. Current Neurology and Neuroscience Reports, 19, 1-12. https://doi.org/10.1007/s11910-019-0917-z
Stern, Y. (2021). How Can Cognitive Reserve Promote Cognitive and Neurobehavioral Health? Archives of clinical neuropsychology: the official journal of the National Academy of Neuropsychologists, 36 7, 1291-1295. https://doi.org/10.1093/arclin/acab049
Tan, J., & Tan, C. (2023). Low neighborhood deprivation buffers against hippocampal neurodegeneration, white matter hyperintensities, and poorer cognition. GeroScience, 1-10. https://doi.org/10.1007/s11357-023-00780-y
Tan, L., Fu, J., Shin, S., & Lee, J. (2022). Association between the mediterranean diet and cognitive health among healthy adults: A systematic review and meta-analysis. Frontiers in Nutrition, 9. https://doi.org/10.3389/fnut.2022.946361
Thompson, L. (2024). Digital Assessment Approaches to Overcome Barriers to Cognitive Screening and Monitoring for Older Adults in Primary Care Settings. Alzheimer's & Dementia, 20. https://doi.org/10.1002/alz.095393
Veeroja, P., Sugiyama, T., Kato, Y., Jamei, E., Abe, T., Sugiyama, M., Chau, H., & Mori, K. (2022). Third Places for Older Adults' Social Engagement: A Scoping Review and Research Agenda. The Gerontologist. https://doi.org/10.1093/geront/gnac180
Warhurst, R., & Black, K. (2024). Theorising Later-Career as a Basis for Enhancing Inclusion and Extending Working Lives Through Human Resource Development. Human Resource Development Review, 23, 522 - 544. https://doi.org/10.1177/15344843241269166
Webb, A., Fallon, J., Page, J., & Babcock, K. (2021). Adult Hippocampal Neurogenesis in Aging and Alzheimer's Disease. Stem Cell Reports, 16, 681 - 693. https://doi.org/10.1016/j.stemcr.2021.01.019
Yu, D., Chan, D., Fong, D., Yu, A., Cheng, C., Bernal, J., & Siu, P. (2022). Effects of exercise intensity and frequency on improving cognitive performance in middle-aged and older adults with mild cognitive impairment: A pilot randomized controlled trial on the minimum physical activity recommendation from WHO. Frontiers in Physiology, 13. https://doi.org/10.3389/fphys.2022.1021428
Zhong, S., Foster, M., Lee, C., & Bian, J. (2020). Intergenerational communities: A systematic literature review of intergenerational interactions and older adults' health-related outcomes. Social science & medicine, 264, 113374. https://doi.org/10.1016/j.socscimed.2020.113374
Zorec, R., & Verkhratsky, A. (2024). Neuroglia in cognitive reserve. Molecular Psychiatry, 29, 3962 - 3967. https://doi.org/10.1038/s41380-024-02644-z
FINANCING
The authors did not receive funding for the development of this research.
CONFLICT OF INTEREST STATEMENT
The authors declare that there is no conflict of interest.
ACKNOWLEDGMENTS
The team of authors would like to thank the Master's Program in Clinical and Educational Neuropsychology at the University of Camagüey "Ignacio Agramonte Loynaz" for their guidance. The first author would especially like to thank the Master's faculty for the excellent training they received.
AUTHORSHIP CONTRIBUTION
Conceptualization: Diego D. Díaz Guerra.
Data curation: Alicia Lianne García González, Diego D. Díaz Guerra, Zoylen Fernández Fleites and Yunier Broche Pérez.
Formal analysis: Alicia Lianne García González, Diego D. Díaz Guerra, Zoylen Fernández Fleites and Yunier Broche Pérez.
Research: Alicia Lianne García González, Diego D. Díaz Guerra, Zoylen Fernández Fleites and Yunier Broche Pérez.
Methodology: Alicia Lianne García González, Diego D. Díaz Guerra, Zoylen Fernández Fleites and Yunier Broche Pérez.
Project management: Alicia Lianne García González, Diego D. Díaz Guerra, Zoylen Fernández Fleites and Yunier Broche Pérez.
Resources: Alicia Lianne García González, Diego D. Díaz Guerra, Zoylen Fernández Fleites and Yunier Broche Pérez.
Software: Diego D. Díaz Guerra.
Supervision: Alicia Lianne García González, Diego D. Díaz Guerra, Zoylen Fernández Fleites and Yunier Broche Pérez.
Validation: Alicia Lianne García González, Diego D. Díaz Guerra, Zoylen Fernández Fleites and Yunier Broche Pérez.
Visualization: Diego D. Díaz Guerra.
Writing - original draft: Diego D. Díaz Guerra.
Writing - proofreading and editing: Alicia Lianne García González, Diego D. Díaz Guerra, Zoylen Fernández Fleites and Yunier Broche Pérez.