Scientific and Technological Research Article
Methodology for the diagnosis of patient pathway management in hospitals
Metodología para el diagnóstico de la gestión de trayectorias de pacientes en hospitales
Yasniel
Sánchez Suárez1 ![]() *,
Maylín Marqués León1
*,
Maylín Marqués León1 ![]() *,
Arialys Hernández Nariño2
*,
Arialys Hernández Nariño2 ![]() *,
María Mayelín Suárez Pérez3
*,
María Mayelín Suárez Pérez3 ![]() *
*
ABSTRACT
The patient flow, referring to the movement of patients through a healthcare institution, is essential for resource optimization, performance enhancement, and satisfaction level elevation within hospitals. The diagnosis of this flow is pivotal as it allows the identification of primary management inefficiencies. This research introduces a methodology structured in five stages for diagnosing patient trajectory management, integrating strategic and operational perspectives. After its implementation in a General Surgery service of a second-level hospital, its applicability was validated. The key deficiencies detected were grouped into essential variables for patient flow management. This methodology offers a holistic approach for healthcare administrators to evaluate the patient's journey within the hospital setting comprehensively.
Keywords: management diagnostics, patient flow, hospital management, process management, management methodology.
Clasificación JEL: I19; M11; M54
RESUMEN
El flujo de pacientes, que se refiere al movimiento de estos a través de una institución sanitaria, es esencial para la optimización de recursos, mejora del rendimiento y elevación de los niveles de satisfacción en hospitales. El diagnóstico de este flujo es crítico, ya que permite identificar deficiencias primarias en la gestión. Esta investigación propone una metodología estructurada en cinco etapas para el diagnóstico de la gestión de las trayectorias de pacientes, integrando perspectivas estratégicas y operativas. Tras implementarla en un servicio de Cirugía General de un Hospital de segundo nivel, se validó su aplicabilidad. Las deficiencias clave detectadas se agruparon en variables esenciales para la gestión del flujo de pacientes. Esta metodología proporciona un enfoque holístico para que los administradores sanitarios evalúen, de manera integral, la trayectoria del paciente dentro del entorno hospitalario.
Palabras clave: diagnóstico de gestión, flujo de pacientes, gestión hospitalaria, gestión de procesos, metodología de gestión.
Received: 03-14-2023 Revised: 25-05-2023 Accepted: 15-16-2023 Published: 04-07-2023
Editor: Carlos Alberto Gómez Cano ![]()
1 Universidad de Matanzas. Matanzas, Cuba.
2 Universidad de Ciencias Médicas de Matanzas. Matanzas, Cuba.
3 Policlínico José Machado. Unión de Reyes, Cuba.
Cite as: Sánchez, Y., Marqués, M., Hernández, A. y Suárez, M. (2023). Metodología para el diagnóstico de la gestión de trayectorias de pacientes en hospitales. Región Científica, 2(2), 2023115. https://doi.org/10.58763/rc2023115
INTRODUCTION
The quality of health services has become a necessity in government management over time, an element that has driven projects to develop quality based on patient satisfaction (Di Fabio et al., 2020; Salas, 2021). In this sense, healthcare should be understood as a public good in constant development, which influences a country's development and growth by contemplating social and economic aspects (Sanchez, 2017). Health services must be organized correctly to meet the population's expectations (Ferrer & Morejón, 2021) through a vision of processes regarding expected results.
Hospital facilities within health services provide medical and nursing care in the specialties defined by their corporate purpose, work 365 days a year, 24 hours a day, and also provide inpatient, outpatient, and emergency services, an element that demonstrates the need for solid process management tools (Morejón, 2022). The national literature (Cuba) identifies contributions to improve the management of hospital organizations (Table 1), of which only one focuses on the management of patient trajectories (PWM) and proposes a specific procedure for the analysis of trajectories (Sánchez, 2023), which is taken as the primary theoretical and methodological reference.
|
Table 1. Contributions to hospital management |
|
|
(Author, year) |
Contribution |
|
(Hernández, 2010) |
Contextualizes the main tools of process management for health services and proposes a tool to evaluate the performance of processes in the hospital. |
|
(García, 2011) |
It proposes tools for the management of human resources with the objective of demonstrating their influence on the improvement of the quality of care. |
|
(Delgado, 2013) |
Procedure for the improvement of the decision-making process by means of operations research tools. |
|
(Marqués et al., 2017) |
Contextualizes the main elements related to the capacity from the strategic to the operative levels of hospital services, to plan supplies of medicines and medical materials. |
|
(García et al., 2019) |
It focuses on a technology that allows evaluating the quality of warehouse management in hospitals. |
|
(Vega de la Cruz, 2020) |
It proposes a set of tools to integrate the processes of the companies with their internal control system. |
|
(Ramos, 2022) |
Proposes a model focused on evaluating the performance of teaching processes in medical science entities. |
|
(Abad, 2022) |
Model for measuring intangible elements. |
|
(Sánchez, 2023) |
Model for the management of patient flows. |
Source: own elaboration.
In hospitals, patients move through the different stages of treatment to receive care (Carnota, 2016); this movement is known in the literature as patient flow, patient trajectory, patient movement, or patient routes. In this regard, Machado (2022) defines patient flow as the path (trajectory, displacement) of patients through the different services involved in their treatment and according to the established medical protocols, with an adequate order in care and optimizing waiting and stay times. The root cause of flow problems is the way they are managed. In this regard, Velásquez et al. (2011) identify the main problems as the accumulation of patients in corridors and on-call corps, long waiting times for care, and days of stay.
Consequently, for the management and improvement of patient trajectories, hospital system tools such as triage (Hughes & Mathai, 2023), the use of maps and signage (Pryce et al., 2021), the use of a flow coordinator (Sánchez et al..., 2023), and different tools from manufacturing have also been contextualized and adapted, including discrete event simulation models (Basaglia et al., 2022), lean manufacturing (Tlapa et al., 2020), system dynamics (Nazarian-Jashnabadi et al., 2023), and capacity management tools, as an expression of the deployment of operations management tools in the sector (Sanchez et al., 2022).
Improving TPM ensures that healthcare organizations optimize their resources during treatment (Dauncey et al., 2022) and alleviates the burden on staff, which brings about continuous improvement in clinical safety and individual patient outcomes (Brosinski & Riddell, 2020); in achieving this objective it is necessary to know the key variables that influence TPM, Sanchez (2023) identifies and defines seven key variables, these are: sequence of activities, focus on the trajectory, system capacity, service demand, computerization, staff qualification and contingency policy, the latter with cross-cutting nature concerning the first six.
Although tools have been developed to diagnose management or analyze flows through the hospital institution (Andersen, 2023; Lee et al., 2022), methodological procedures still need to be improved for specialists and staff in charge to identify the causes and sub-causes of management deficiencies correctly. Consequently, the objective of the research is to design a methodology for the diagnosis of TPM in hospitals.
METHODS
The research is quantitative, based on an analytical, non-experimental study in a clinical-surgical teaching hospital in Cuba to diagnose PWM. A methodology for its analysis is proposed (Figure 1), composed of five stages; the first three stages will give a strategic vision of the institution, essential elements to take into account to identify possible origins of the flows, level of complexity, and possible stages of treatment, which in turn are of importance for management, and two stages that show a more operational vision of the patient's trajectory through key processes for management.
The research was carried out in the General Surgery service of the hospital selected as the object of study. Although the selection was not probabilistic, according to Gómez et al. (2022), it was recommended by the entity's board of directors due to the significant influence of this service on the overall performance of the institution and its ability to address the trajectories of both elective and emergency patients.
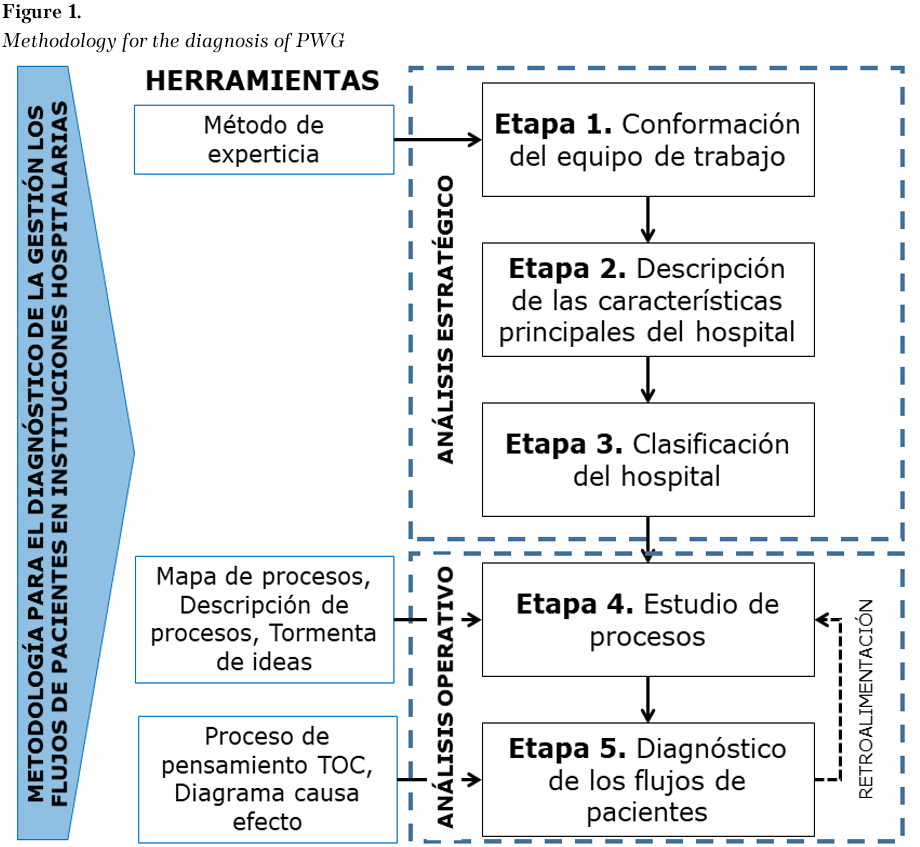
Source: own elaboration.
Note: the figure appears in its original language.
Description of the methodology
Stage 1. Formation of the work team
The objective was to form a work team with members from the different key result areas of the hospital institution, which would provide a process vision of the PWM (stage of treatment through which the patient must pass in the service). In their selection, their level of expertise in their task was considered; the research used the method proposed by Artola (2002).
The coefficient of expertise (EI) is calculated with equation 1, an indicator that depends on the level of knowledge (K) possessed by the members of the work team (equation 2) in terms of:
· Theoretical or experimental knowledge (weight: 0.30),
· Practical knowledge (weight: 0.50),
· National bibliography consulted (weight: 0.05),
· International bibliography consulted (weight: 0.05),
· Knowledge of the problem (weight: 0.05),
· Intuition (weight: 0.05).
Where:
· Wj: weight of the criterion (these criteria can be modified and the weights recalculated).
· Kc: Knowledge coefficient.
· Ka: argumentation coefficient.
· n: number of experts to integrate the work team.
Note: the value of K must be between 0.70 and 1.00 for the expert to be considered competent.
Stage 2. Description of the main characteristics of the hospital
The characterization of the hospital was carried out based on the 13 variables, which are contextualized in their application to the health services sector by Hernández et al. (2014). The variables are: limit and boundary (1), medium or environment (2), strategic analysis (3), processes (4), service portfolio (5), transformation (6), business resources (7), stability (8), results (9), feedback and control (10), flexibility (11), inertia (12) and hierarchy (13).
Stage 3. Hospital classification
Each hospital has unique characteristics determined by its profile, the services it offers, its geographic location -which defines its scope- and its capacity, reflected in the number of beds available to meet patient demand and maintain an adequate standard of service. These categories are not mutually exclusive. The critical criteria used in the research include profile, location, and number of beds, as these are the factors with the most significant impact on PWM.
Step 4. Process study
The experts used the institution's process map to select the processes to be investigated. This tool facilitated the visualization of the categorized processes (critical, strategic, and support) and their interconnections. This allowed them to identify the elements with the most significant impact on flows and to explore opportunities for integration and collaboration in patient care.
Once the process was selected, it was described and represented. In the research, the cross-functional diagram was used, which highlighted the interaction between various processes throughout the different phases of patient care.
Stage 5. Diagnosis of patient flows
For the diagnosis of patient flows, the TOC (Theory of Constraints) thought process was used; its thought process diagram is shown in figure 2.
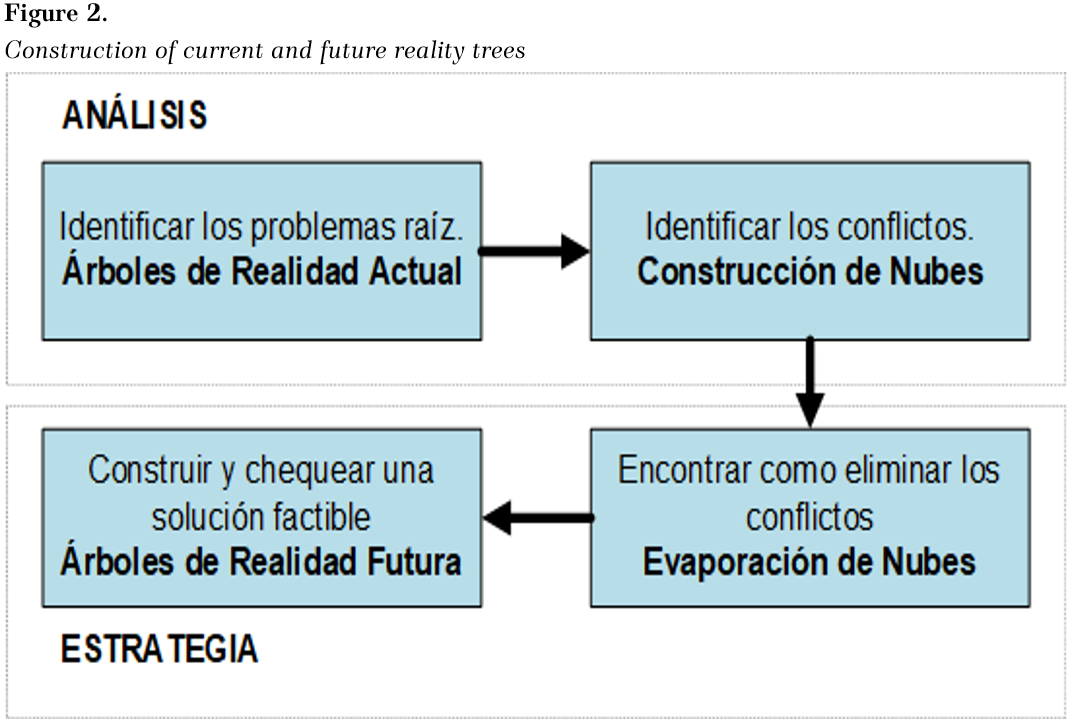
Source: own elaboration.
Note: the figure appears in its original language.
In order to draw up the current reality tree, participatory observation of processes was used. This methodology made it possible to identify deficiencies linked to service flows. Once identified, their cause-effect relationships were analyzed. Each deficiency detected at the beginning of the tree is labeled as a 'root cause.' If a deficiency accumulates the highest number of related problems, it is called a 'root problem.'
The 'conflict cloud' is a technique that, through teamwork, facilitates the resolution of conflicts identified as deficiencies. On the other hand, the 'future reality tree' visualizes desired or projected states achieved after implementing corrective actions, also known as 'injections.' This tree integrates various improvement-oriented techniques, procedures, and methodologies.
Several cause-effect relationships were discovered as we progressed through this stage, providing a systemic view of the process essential for effective management. In addition, thanks to the application of cause-effect diagrams, it was possible to synthesize the root causes and reorganize them according to key variables that impact TPM.
The following results were obtained from the application of the proposed methodology for the diagnosis of PWM in hospitals:
Stage 1. Formation of the work team
The work team was structured with 10 experts and their experience was verified (Table 2).
|
Table 2. Proposed team experts |
|||||
|
No. of experts (Exp.) |
Working Time (years) |
Kc |
Ka |
K |
Competition |
|
Exp. 1 |
29 |
1.00 |
0.86 |
0.93 |
Competent |
|
Exp. 2 |
26 |
1.00 |
0.86 |
0.93 |
Competent |
|
Exp. 3 |
11 |
0.86 |
0.90 |
0.88 |
Competent |
|
Exp. 4 |
30 |
0.86 |
0.74 |
0.87 |
Competent |
|
Exp. 5 |
33 |
1.00 |
0.90 |
0.95 |
Competent |
|
Exp. 6 |
26 |
1.00 |
0.86 |
0.93 |
Competent |
|
Exp. 7 |
46 |
1.00 |
0.88 |
0.95 |
Competent |
|
Exp. 8 |
30 |
1.00 |
0.90 |
0.94 |
Competent |
|
Exp. 9 |
32 |
1.00 |
0.84 |
0.92 |
Competent |
|
Exp. 10 |
16 |
0.74 |
0.94 |
0.86 |
Competent |
Source: own elaboration.
Stage 2. Description of the main characteristics of the hospital
The 13 variables for the characterization were deployed:
1. Limit and boundary: The hospital under study is public and is part of the national health system; it integrates the second level of care and supports the primary level; it is accredited as a science and technology unit.
2. Environment: It serves the population of the territory and foreigners who require care. The leading suppliers are wholesale drug companies, electromedical workshops, provincial health directorate, and logistics companies.
3. Strategic analysis: The mission, vision, and strategic objectives defined in the institution are redesigned based on future institutional accreditation cycles.
4. Processes: The strategic or hospital governance processes, the key or assistance processes, and the support processes that influence organizational functioning are defined. The main processes identified are hospitalization, clinical-surgical, and teaching.
5. Portfolio of services: The entity provides services in 36 specialties, including clinical, surgical, and emergency treatments.
6. Transformation: The transformation is developed from the fact that patients receive medical care and evolve or not the condition for which they demand the service.
7. Business Resources: The primary business resources are human resources (health specialists and support staff), financial, material, managerial, intangible and infras, and structure.
8. Stability: The hospital has stability levels of 85% and is constantly strengthening its processes.
9. Results: structured protocols, treatments, medication, food, energy, financing, and equipment.
10. Feedback and control: monitoring of strategic indicators.
11. Flexibility: The institution adapts easily to changes regulated by the health system, for which it has designed a risk prevention plan based on the uncertainty of demand and the food distribution and supply systems.
12. Inertia: continues as a leader in patient care by consolidating its processes and organizational culture.
13. Hierarchy: It is structured in three levels: management, vice management, and services or departments.
Stage 3. Hospital classification
The provincial-level, clinical-surgical teaching hospital provides outpatient, emergency, and inpatient medical services. It has 418 beds, of which 356 are currently in use. It has state-of-the-art equipment. Its human resources are in the order of 1,859, including specialists and support staff. Out of its 36 medical specialties, they function as teaching units.
Stage 4. Process study
Based on the analysis of the institution's process map and after consulting with specialists, the team decided to focus its study on the hospitalization process, which is the central pillar of the hospital. The health statistical yearbooks from 2018 to 2021 were examined to choose the specific service, focusing on surgical activity (see Table 3). The General Surgery service was chosen, which recorded 7,452 surgical interventions in 2020, equivalent to 26.3% of the total. It is worth noting continued growth in 2018 and 2019. However, the prevalence of this service has always been remarkably high.
|
Table 3. Analysis of surgical activity |
||||
|
Surgical activity |
Years |
|||
|
2018 |
2019 |
2020 |
2021 |
|
|
Other specialties |
11672 |
13150 |
7452 |
4982 |
|
Cardiovascular surgery, angiology and endovascular surgery |
1451 |
482 |
164 |
36 |
|
Otorhinolaryngology |
974 |
3596 |
1533 |
723 |
|
Orthopedics |
2975 |
5607 |
1982 |
745 |
|
Gynecobstetrics |
171 |
5923 |
2327 |
1322 |
|
Urology |
2219 |
11904 |
7143 |
3033 |
|
General surgery |
6152 |
18271 |
7452 |
2906 |
Source: own elaboration.
Note: the figure appears in its original language
General surgery services have a low bed turnover and a high hospital stay associated mainly with the complexity of surgical procedures. This highlights the relevance of the analysis of patient trajectories. The cross-function diagram was used for its representation (figure 3).
Figure 3.
Cross-function diagram: General Surgery services
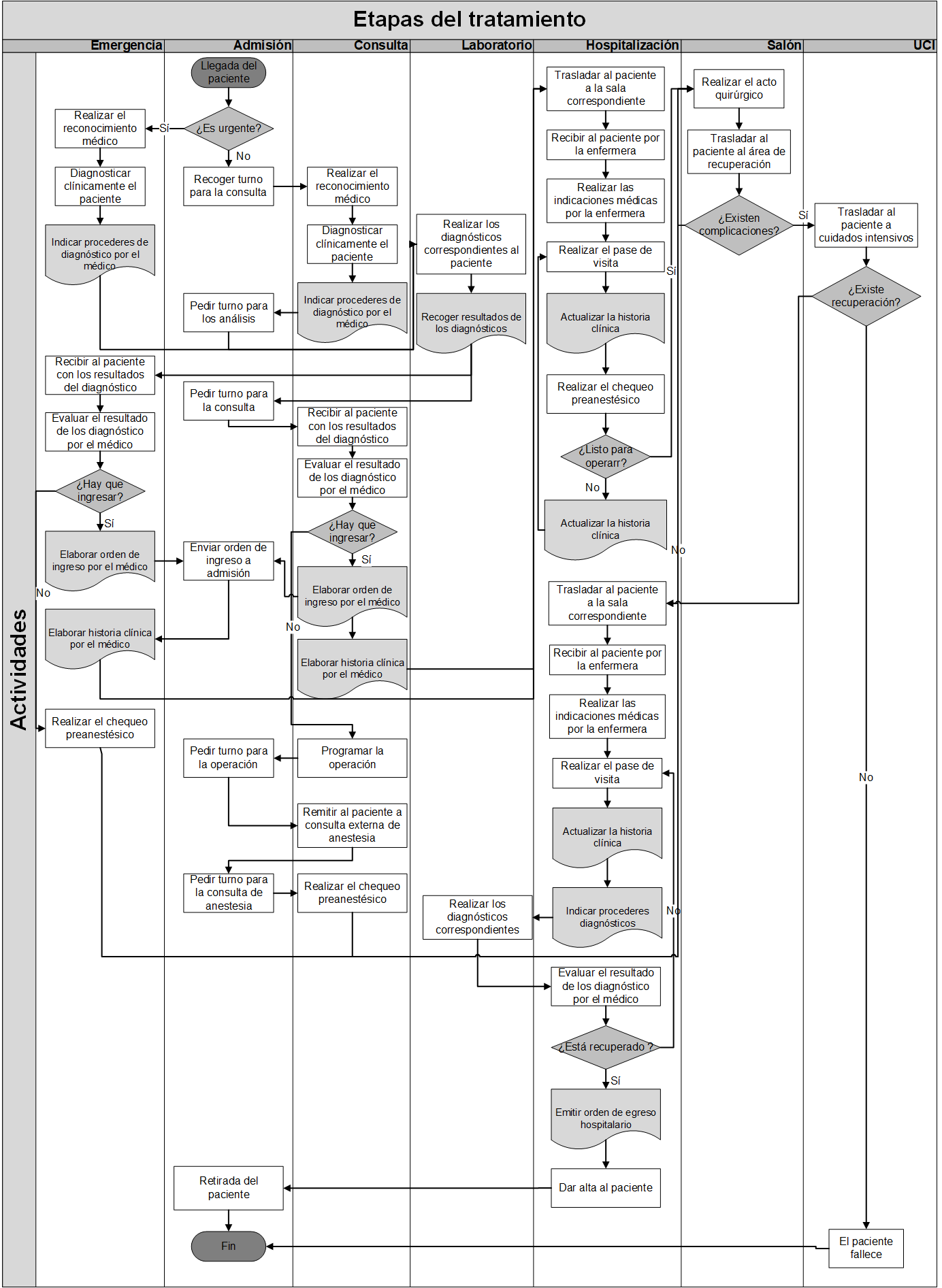
Source: own elaboration.
Note: the figure appears in its original language.
Stage 5. Diagnosis of patient flows
In a work meeting with the team of experts, a brainstorming session was held to identify the primary deficiencies, their cause-effect relationships, and possible future solutions based on the conception of the origin of the conflict (figure 4).
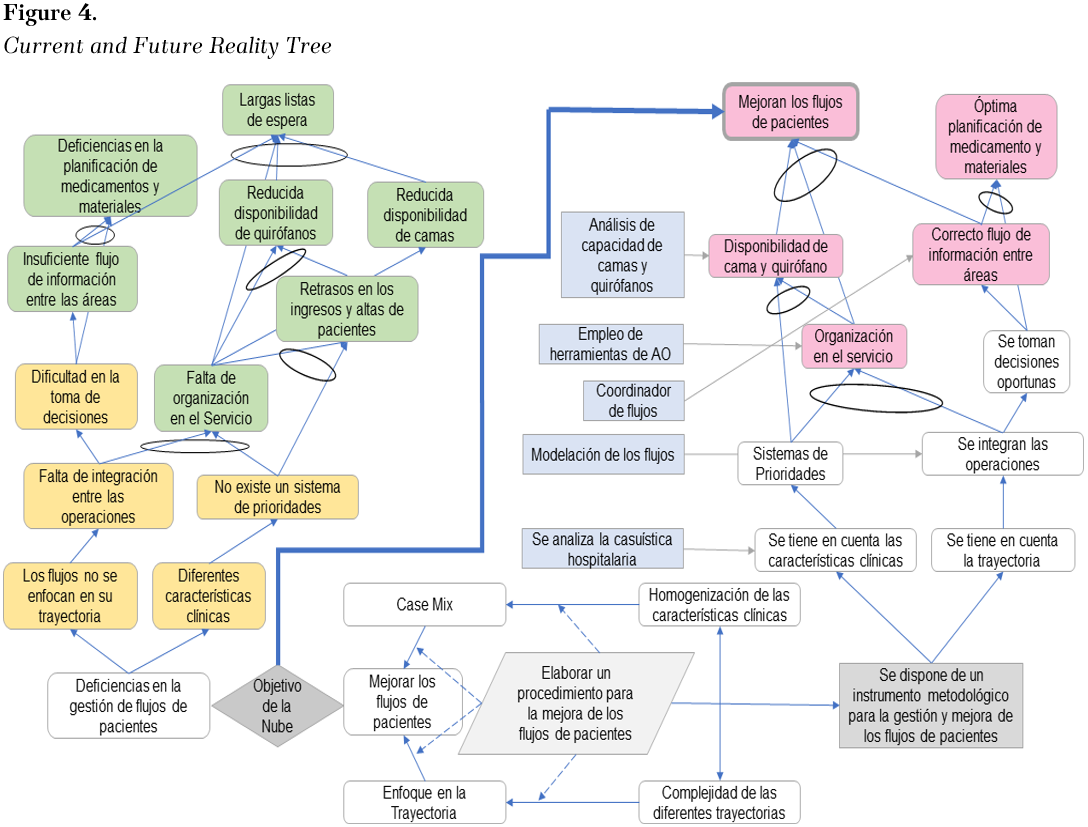
Source: own elaboration.
Note: the figure appears in its original language.
The root problem was identified as deficiencies in PWM in the service, and the set of causes related to it were prioritized based on the application of the Kendall method. Structured brainstorming sessions were conducted to identify sub-causes and classify them into internal and external sub-causes to the service. Using affinity diagrams, these causes and subcauses were related to the key variables that influence the TPM (Figure 5).
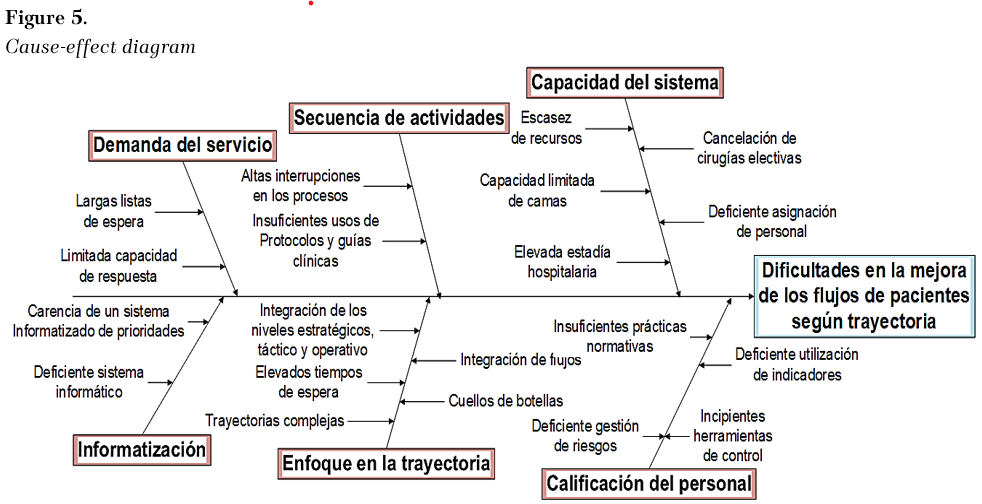
Source: own elaboration.
Note: the figure appears in its original language.
Diagnosing patient trajectories and identifying causes and subclauses that affect their efficiency made it possible to implement measures that optimize these trajectories. This optimization reduces waiting times and average length of stay, enhancing hospital performance.
In the literature, there is evidence of contributions to the diagnosis of management and analysis of patient trajectories. In correspondence with the research, Giron (2021) recognizes the need for the analysis of flows in terms of improvement; in his research, they apply as a diagnostic method the current value flow maps in an emergency unit of pediatric patients; in turn, Hernandez et al. (2017) perform an analysis in an emergency department from the application of discrete simulation techniques.
In addition to the above, Martínez and Duarte (2020) analyze a chemotherapy service in a public organization using mathematical modeling, research that corresponds with that of Hernández et al. (2017). These authors rely on mathematical simulation models to analyze and evaluate flows. These methods, although compelling, need highly qualified personnel for their deployment, application, and monitoring over time.
Consequently, authors such as Torres and Velasco (2020) apply the Business Process Management (BPM) methodology and lean tools in order to eliminate all those activities that do not generate value in the treatment of the patient, a methodology that, although it takes into account process management, as in the research, does not show the procedure to perform this analysis from the strategic to the operational levels.
Among the positive implications for the hospital institution are:
1. It allows to optimize the capacity by reducing the patient's length of stay.
2. To count on a proactive diagnosis of the behavior of the TPM, an element that influences patient satisfaction, by identifying interruptions and reducing waiting times.
3. Increases collaboration between processes by showing the possibility of management from strategic to operational levels.
4. Increases hospital performance by focusing on the patient's trajectory and reducing the length of stay, elements that influence the pace of care, optimization of human resources and bed turnover levels.
CONCLUSIONS
A five-step structured methodology was developed to diagnose TPM in hospital settings. This methodology incorporates several tools, including a rigorous selection of experts based on verification of their expertise, process mapping and representation, the TOC Thought Process approach, and cause-effect diagramming. This holistic approach allows healthcare managers to comprehensively assess the management of patient flows, focusing attention on their journey through the hospital.
Practical application of the methodology in the General Surgery service confirmed its usefulness and relevance. The process was broken down using a cross-functional diagram, and primary deficiencies associated with PWM were identified using the TOC Thinking Process.
Among the study's limitations is training the selected experts to ensure familiarity with crucial flow concepts. This training would be essential to standardize language among team members and researchers, ensuring cohesive work. Future research suggests designing a training strategy and exploring additional tools for the effective diagnosis of PWM in hospital settings.
REFERENCES
Abad, A. (2022). Modelo de medición de elementos intangibles y su procedimiento de implementación en el sector de la salud. Caso de estudio Hospital Provincial Docente Clínico Quirúrgico Faustino Pérez de Matanzas [Tesis de Doctorado, Universidad de Matanzas]. Repositorio UMCC. https://rein.umcc.cu/handle/123456789/1373
Andersen, A. (2023). Evaluation of patient flow and other queueing systems with relocation. Software Impacts, 17, 100528. https://doi.org/10.1016/j.simpa.2023.100528
Artola, M. (2002). Modelo de evaluación del desempeño de empresas perfeccionadas en el tránsito hacia empresas de clase en el sector de servicios ingenieros de Cuba [Tesis de Doctorado, Universidad de Matanzas]. Repositorio UMCC. http://scholar.google.com/scholar?cluster=13499215808066917373&hl=en&oi=scholarr
Basaglia, A., Spacone, E., Van de Lindt, J. y Kirsch, T. (2022). A Discrete-Event Simulation Model of Hospital Patient Flow Following Major Earthquakes. International Journal of Disaster Risk Reduction, 71, 102825. https://doi.org/10.1016/j.ijdrr.2022.102825
Brosinski, C. y Riddell, A. (2020). Incorporating Hourly Rounding to Increase Emergency Department Patient Satisfaction: A Quality Improvement Approach. Journal of Emergency Nursing, 46(4), 511-517. https://doi.org/10.1016/j.jen.2019.08.004
Carnota, O. (2016). La irrupción de la gerencia en las organizaciones sanitarias del sector público. Rev Cubana Salud Pública, 42(4), 596-627. https://www.scielosp.org/article/rcsp/2016.v42n4/596-627
Dauncey, S., Kelly, P., Baykov, D., Skeldon, A. y Whyte, M. (2022). Rhythmicity of patient flow in an acute medical unit: relationship to hospital occupancy, 7-day working and the effect of COVID-19. QJM: An International Journal of Medicine, 114(11), 773-779. http://doi.org/10.1093/qjmed/hcaa334
Delgado, A. (2013). Herramientas de la Investigación de Operaciones para abordar problemas de decisión en el proceso quirúrgico del Hospital Julio M. Aristegui Villamil [Tesis de Maestría, Universidad de Matanzas]. Repositorio UMCC. https://rein.umcc.cu/handle/123456789/233
Di Fabio, J., Gofin, R. y Gofin, J. (2020). Análisis del sistema de salud cubano y del modelo atención primaria orientada a la comunidad. Revista Cubana de Salud Pública, 46, e2193. https://www.scielosp.org/article/rcsp/2020.v46n2/e2193/
Ferrer, Y. y Morejón, Y. (2021). Gestión intersectorial, herramienta para la gestión de políticas públicas. Una experiencia cubana en la atención primaria de salud. Panorama Cuba y Salud, 16(2), 142-145. https://revpanorama.sld.cu/index.php/panorama/article/download/1113/pdf
García, D., Cedeño, Y., Ríos, I. y Morell, L. (2019). Índice integral de calidad para la gestión de almacenes en entidades hospitalarias. Gaceta Médica Espirituana, 21(1), 21-33. http://scielo.sld.cu/pdf/gme/v21n1/1608-8921-gme-21-01-21.pdf
García, V. (2011). Procedimiento para la implementación de la Gestión del Capital Humano en servicios asistenciales de hospitales [Tesis de Doctorado, Instituto Superior Politécnico José Antonio Echeverría (CUJAE)]. Repositorio UACA. https://catalogo.uaca.ac.cr/cgi-bin/koha/opac-detail.pl?biblionumber=228051
Girón, E. (2021). Cadena y Mapa de Flujo de Valor para Modelo de Pacientes Pediátricos Urgentes-Emergentes (Modelo PPUE): Caso Pandemia de Coronavirus. Academia Journals, 13(2), 103-111. https://goo.su/XDLt
Gómez, C., Sánchez, V., Ballen, Y. y Bermúdez, M. (2022). Análisis de los riesgos asociados a la prestación de servicios en sala de enfermedades respiratorias durante la pandemia COVID-19 en el Hospital Maria Inmaculada. Salud, Ciencia y Tecnología, 2(123), 1-7. https://doi.org/10.56294/saludyt2022123
Hernández, A. (2010). Contribución a la gestión y mejora de procesos en instalaciones hospitalarias del territorio matancero [Tesis de Doctorado, Universidad de Matanzas]. Repositorio UMCC. https://rein.umcc.cu/handle/123456789/24
Hernández, A., Medina, A., Nogueira, D., Negrín, E. y Marqués, M. (2014). La caracterización y clasificación de sistemas, un paso necesario en la gestión y mejora de procesos. Particularidades en organizaciones hospitalarias. Dyna, 81(184), 193-200. http://www.redalyc.org/articulo.oa?id=49630405027
Hernández, D., Camacho, M. y Duarte, E. (2017). Análisis del flujo de pacientes en el servicio de urgencias del Hospital Universitario la Samaritana a través de simulación discreta. AVANCES Investigación en Ingeniería, 14(1), 109-122. http://doi.org/10.18041/1794-4953/avances.1.1289
Hughes, B. y Mathai, M. (2023). EPNS4Surge: an MDT-designed integrated learning course facilitating effective patient flow from triage to discharge. Science Talks, 5, 100128. https://doi.org/10.1016/j.sctalk.2023.100128
Lee, S., Shin, S., Ro, Y., Lee, H. y Yoon, J. (2022). Multimodal Quality Improvement Intervention With Dedicated Patient Flow Manager to Reduce Emergency Department Length of Stay and Occupancy: Interrupted Time Series Analysis. Journal of Emergency Nursing, 48(2), 211-223.e213. https://doi.org/10.1016/j.jen.2021.12.001
Machado, L. (2022). Papel de la ingeniería industrial dentro de las disciplinas que permiten asegurar servicios de salud de calidad. Revista Cubana de Salud Pública, 48(Supl. revisiones), e2195. https://revsaludpublica.sld.cu/index.php/spu/article/download/2195/1826
Marqués, M., Negrin, E., Hernández, A., Nogueira, D. y Medina, A. (2017). Modelo para la planificación de medicamentos y materiales de uso médico en instituciones hospitalarias. Gestión y política pública, 26(SPE), 79-124. http://www.scielo.org.mx/scielo.php?script=sci_arttext&pid=S1405-10792017000300079
Martínez, H. y Duarte, E. (2020). Análisis del flujo de pacientes utilizando la simulación discreta en una unidad de quimioterapia de una organización sin ánimo de lucro. Inventum, 15(29), 23-36. http://doi.org/10.26620/uniminuto.inventum.15.29.2020.23-36
Morejón, M. (2022). Análisis del impacto de los indicadores de gestión hospitalaria en el funcionamiento administrativo de una institución de salud en Ensenada, B.C. [Tesis de Maestría, Universidad Autóctona de Baja California]. Repositorio UABC. http://repositorioinstitucional.uabc.mx/server/api/core/bitstreams/34f0df3a-492b-4779-a9a5-fac6830fffb7/content
Nazarian-Jashnabadi, J., Rahnamay, S., Haseli, G., Tomaskova, H. y Hajiaghaei-Keshteli, M. (2023). A dynamic expert system to increase patient satisfaction with an integrated approach of system dynamics, ISM, and ANP methods. Expert Systems with Applications, 234, 121010. https://doi.org/10.1016/j.eswa.2023.121010
Pryce, A., Unwin, M., Kinsman, L. y McCann, D. (2021). Delayed flow is a risk to patient safety: A mixed method analysis of emergency department patient flow. International Emergency Nursing, 54, 100956. https://doi.org/10.1016/j.ienj.2020.100956
Ramos, G. (2022). Gestión del desempeño del Sistema de Ciencia e Innovación enfocado a los procesos académicos en Salud [Tesis de Doctorado, Universidad de Matanzas]. Repositorio UMCC. https://rein.umcc.cu/handle/123456789/1486
Salas, J. (2021). Políticas Públicas para mejorar la calidad de servicios de salud. Ciencia Latina Revista Científica Multidisciplinar, 5(1), 253-266. http://doi.org/10.37811/cl_rcm.v5i1.223
Sánchez, D. (2017). Accesibilidad a los servicios de salud: debate teórico sobre determinantes e implicaciones en la política pública de salud. Revista Médica del Instituto Mexicano del Seguro Social, 55(1), 82-89. http://www.redalyc.org/articulo.oa?id=181529929002
Sánchez, Y. (2023). Instrumento metodológico para la gestión de trayectoria de pacientes en instituciones hospitalarias [Tesis de Doctorado, Universidad de Matanzas]. Repositorio UMCC. https://rein.umcc.cu/handle/123456789/1949
Sánchez, Y., Estupiñán, S., Marqués, M., Hernández, A. y Medina, A. (2022). Descripción de prácticas de administración de operaciones aplicadas a la gestión de servicios hospitalarios: un análisis de la literatura. Ingeniería Industrial, (43), 81-100. http://doi.org/10.26439/ing.ind2022.n43.6110
Sánchez, Y., Lorente, L., Diéguez, E. y Nogueira, D. (2023). Coordinadores de flujo: papel en la gestión de trayectorias de pacientes con coronavirus. Universidad y Sociedad, 15(4), 620-630. http://rus.ucf.edu.cu/index.php/rus/article/download/4019/3933
Sánchez, Y., Marqués, M., Hernández, A. y Santos, O. (2023). Hospital rough cut capacity planning in a General Surgery service. Dyna, 90(25), 45-54. http://doi.org/10.15446/dyna.v90n225.103774
Tlapa, D., Zepeda-Lugo, C., Tortorella, G., Baez-Lopez, Y., Limon-Romero, J., Alvarado-Iniesta, A. y Rodriguez-Borbon, M. (2020). Effects of Lean Healthcare on Patient Flow: A Systematic Review. Value in Health, 23(2), 260-273. https://doi.org/10.1016/j.jval.2019.11.002
Torres, G. y Velasco, J. (2020). Aplicación de la metodología BPM e instrumentos Lean para evaluación del flujo de pacientes en el área de servicios quirúrgicos. Estudio de caso: hospitales de alta complejidad. [Tesis de pregrado, Universidad Santo Tomás]. Repositorio USTA. http://hdl.handle.net/11634/31398
Vega de la Cruz, L. (2020). Tecnología para la gestión integrada del control interno con enfoque multicriterio en organizaciones cubanas [Tesis de Doctorado, Universidad de Holguín]. Repositorio ANEC. https://observatorio.anec.cu/detail?id=60637ba151b6a548fa7a902c&type=materials/from=%rFserach
Velásquez, P., Rodríguez, A. y Jaén, J. (2011). Metodologías cuantitativas para la optimización del servicio de urgencias: una revisión de la literatura. Revista Gerencia y Políticas de Salud, 10(21), 11. http://www.scielo.org.co/pdf/rgps/v10n21/v10n21a12.pdf
FINANCING
No external financing.
DECLARATION OF CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
ACKNOWLEDGMENTS (ORIGINAL SPANISH VERSION)
Se agradece a la Universidad de Matanzas y a la coordinadora del proyecto nacional “Perfeccionamiento de los Procesos y la Cadena de Suministro” por el apoyo recibido durante el desarrollo de la investigación.
AUTHORSHIP CONTRIBUTION
Conceptualization: Yasniel Sánchez Suárez, Maylín Marqués León.
Formal analysis: Arialys Hernández Nariño, María Mayelín Suárez Pérez.
Research: Yasniel Sánchez Suárez, Arialys Hernández Nariño.
Methodology: Maylín Marqués León.
Software: Yasniel Sánchez Suárez, María Mayelín Suárez Pérez.
Validation: Yasniel Sánchez Suárez, Maylín Marqués León.
Writing - original draft: Yasniel Sánchez Suárez.
Writing - revision and editing: Maylín Marqués León, Arialys Hernández Nariño.